4.5.24
An elderly patient (c/o Gurmukh Singh, ex-employee, gynae), 70 years of age, presented with epigastric and RUQ symptoms, with previous history of open cholecystectomy at Malerkotla civil hospital through a small incision (so-called mini-lap).

The ultrasound scan, however, still showed a smaller rounded gallbladder.
An MRCP was obtained for local biliary anatomy.

At lap chole, dense omental and colonic adhesions took time to safely dissect off the top of the gallbladder which came into view only at the middle of the gallbladder fossa.
Thereafter, the going was easy.
2.4.24
A 45 years old lady presented with a big painful swelling below the umbilicus which was diagnosed clinically as PUH, possibly obstructed. At operation instead, the swelling turned out to be a chronic abscess full of thick pus. Further exploration showed a foreign body emerging out of a small hole in the rectus sheath, and on enlarging the opening in the sheath, a full sized abdominal pack could be pulled out (gossypiboma). The drain continued to drain thick pus for 3 weeks and then dried out, with full recovery.

19.4.24
Lap chole in a 50 years old female turned out to be very difficult due to dense fibrosis in the Calot’s triangle. She had a very big stone (34 mm on US) impacted in the neck of gallbladder, the stone was disimpacted and removed. Still no safe progress could be made in dissection of the area due to dense fibrosis, and the case was converted to open after 2 hours.
At open operation, the thick mass at the neck of gallbladder could be separated from the underlying bile duct which however was denuded to expose mucosa. The drain in this case continued to drain bile for a little more than 3 weeks and then dried out.

Tuberculosis of the breast
Posted on: May 2, 2024
8.3.24
A 38-year-old lady (Dr Rajni’s patient) presented with a long-standing (more than 6 months duration as per history) inflammatory mass in the left breast – never actually resolving despite prolonged antibiotic treatment and diagnosed clinically as an antibioma. This mass (along with a sinus which had developed recently) was excised under general anesthesia. The biopsy report surprisingly came out to be tuberculosis.


Was referred to TB hospital for medical treatment of tuberculosis. There she was put on anti-tubercular drugs, starting with 4 drug combination for first two months.
Gastrojejunostomy with repair of diaphragmatic eventration, and gallstones with CBD stones
Posted on: May 1, 2024
22.12.23
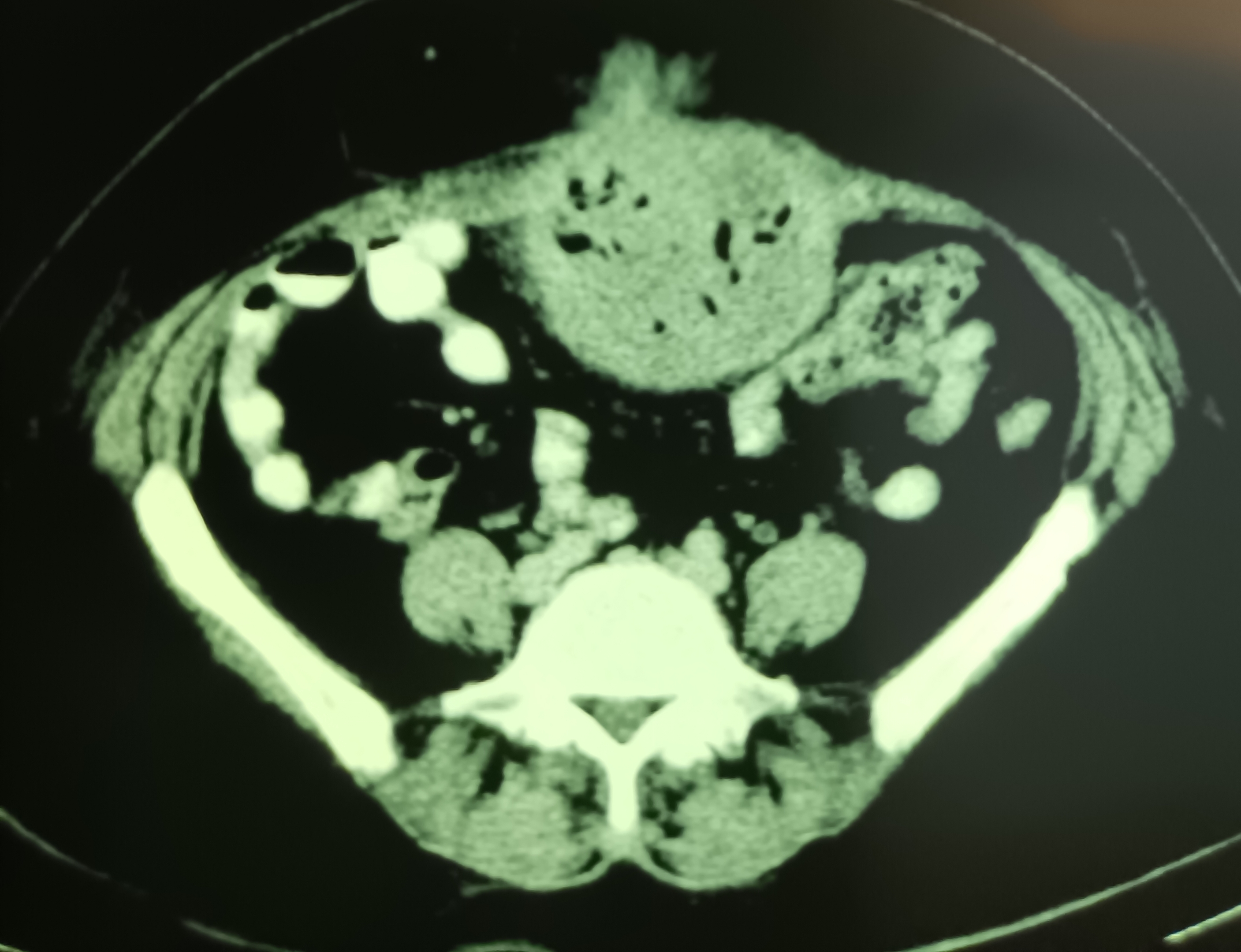
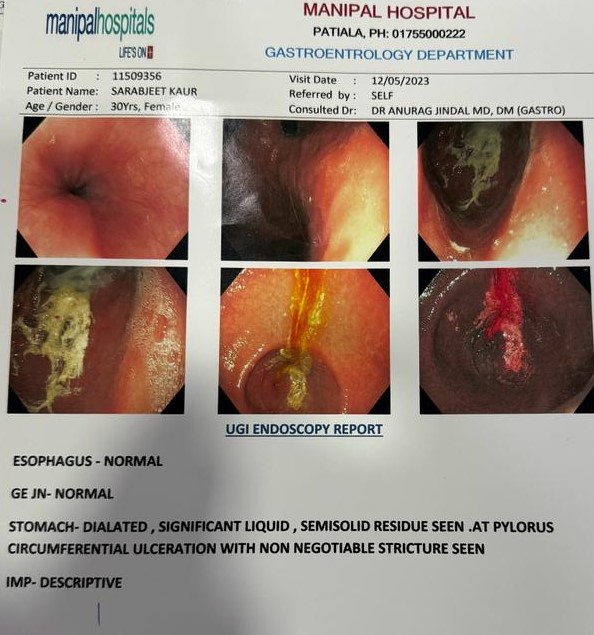
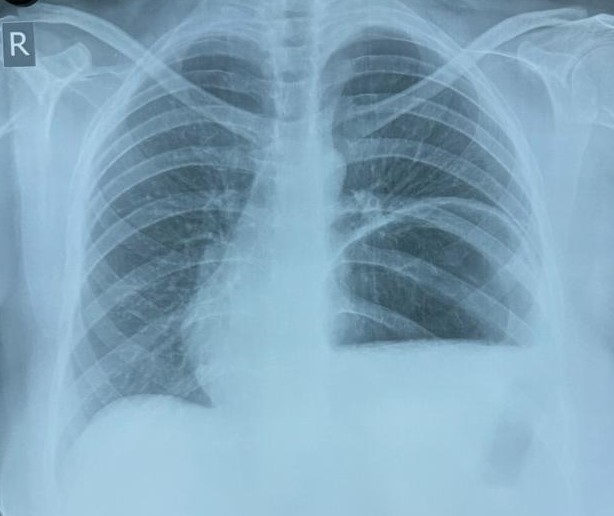
A 35 years old female presented with features of pyloric stenosis/GOO (gastric outlet obstruction) ulcer , confirmed on endoscopy, for which a retrocolic gastrojejunostomy was performed. Also her chest x-ray revealed eventration of diaphragm, for which the diaphragm was plicated with running layers of 1-0 prolene sutures.
25.1.24
A very difficult lap chole was done in a 60 years old male, with history of choledocholithiasis (ERCP showed a meniscus sign) too, for which ERCP clearance had already been done. The procedure took 3 hours, the Calot’s triangle was all fibrotic. Fundus first dissection up to the neck of gallbladder was done and the neck ligated below it with vicryl.
Omentocele stuck to testis, a torticollis, and a bile leak in a difficult LC
Posted on: April 27, 2024
27.9.23
A 28 years old male patient (related to an employee of saket hostpital) presented with torticollis since childhood, with severe deformity of neck and face. The neck X-ray revealed scoliosis, making intubation for anesthesia difficult.
A bipolar sternocleidomastoid tenotomy was performed, and a cervical collar given.
21.10.23
During dissection for a big right inguinal hernia, it was found that the big omentocele was adherent to the testis and appeared to be going into the testis. And indeed, the capsule of the testis had to be incised to deliver the omentum from within the testis.


28.11.23
During a difficult dissection in a lap chole, cautery dissection lower down on the Hartmann pouch resulted in a tiny perforation which resulted in a bile leak for a week.
19.6.2023
RIH indirect hernia repaired in an obese 50 years old male patient. The indirect which was ligated and excised as usual. Also had a big lipoma in the canal quite free from the cord – unusual. This was excised too.
20.6.23
Urethral caruncle in an elderly 65 years old female had caused urinary obstruction and stricture of the distal urethra. Was catheterized after excision of the caruncle and urethral dilatation.
30.6.23
Mesh removal in a 67 years old male (brother of Cheema Sahib Singh) following meshalgia and a chronic sinus developing after a hernia repair in 2022. The mesh was removed with difficulty. The wound developed a hematoma and infection for which the nonhealing wound was laid open on 16.7.23. After this, the wound gradually healed.
9.7.23
A difficult lap chole in a diabetic and hypertensive 55 years old male took more than 2 hours but was eventually successful when the gall bladder was emptied of the big stones first, and the big Hartmann pouch was lifted high up to reveal a fibrotic calot’s triangle. Dissection starting higher up from the left could achieve a plane of dissection behind the neck of gallbladder, at which level it was ligated with vicryl. Earlier attempts at dissecting from the right on the H. pouch were not successful.
Craniectomy bones in the thigh forgotten for more than 10 years, and an abandoned APR for GIST of the rectum
Posted on: September 20, 2023
19.5.23
A 76 years old rural lady had undergone brain aneurysm clipping at PGI in 2010, when the craniectomy bones were kept in a subcutaneous pocket in the thigh. She never reported back there for removal of these bones from the thigh, and forgot about them. Now after 13 years she presented at TNH with a large palpable swelling over the thigh with a discharging sinus. The bones were removed and the wound which had a large collection of serosanguinous fluid cleaned and debrided of several areas of inflammatory granulations, drained and sutured.



27.5.23
A large paraumbilical hernia (supraumbilical) repaired with mesh in a 62 years old hypertensive, diabetic and obese lady (w/o Ranjit S Bhullar). The incarcerated omentum looked like gut loops, eventually dissected out completely and excised. Drain removed after 5 days, but the wound continued to discharge and took exactly a month (till 27 June) to dry up.
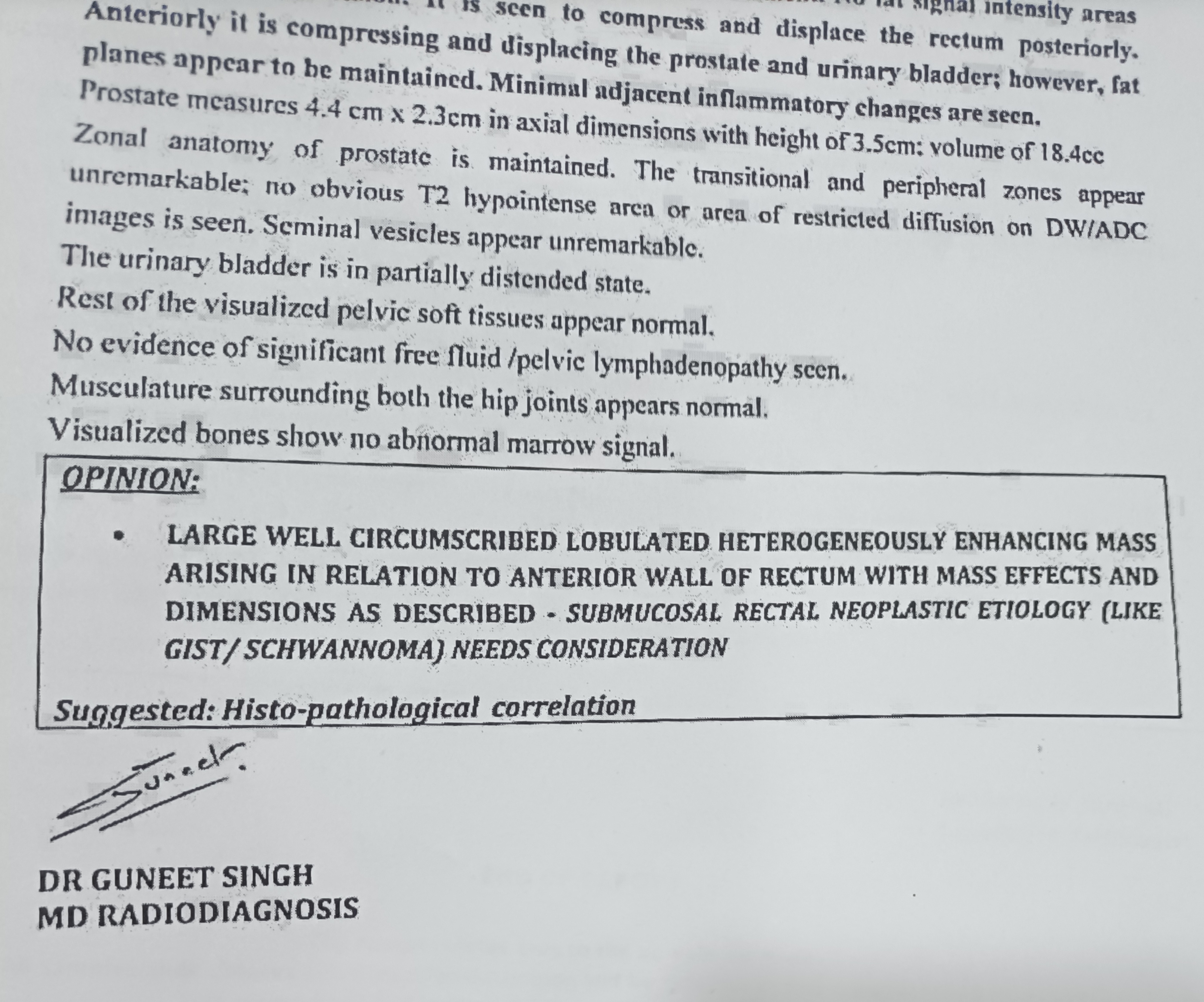
An attempted APR (case of Dr Sukhpreet) was abandoned in favour of palliative sigmoid loop colostomy in a 60 years old male patient, who had a big mass in the rectum diagnosed as GIST (spindle cell type) on biopsy. At exploration, the mass was found to be immobile, with vascular angry-looking surface; and the resection was abandoned. The sigmoid colon was found to be large and fixed in the right side; so had to be mobilised and and a loop colostomy made in the RIF.


Chronic venous leg ulcer, persisting despite multiple interventions; and a breast cancer incorrectly diagnosed
Posted on: August 20, 2023
5.5.23
A 45 years old patient presented with a history of suffering for 5 years from varicose veins and a non-healing ulcer in the right lower leg. Had undergone surgery for varicose veins twice in RHP, first in 2018 and then again in 2020. A third surgery was done in a private hospital in 2023. On examination the ulcer and varicose veins were still present. Was advised a repeat venous doppler ultrasound study, and compression dressings/stockings in the meantime. He never reported back. However, the two prescriptions he carried were the following.


4.5.23
A wide local excision of a breast lump was carried out in a 45 years old female (Dr Jagga’s case), presuming the the lump to be not malignant because the FNAC had not reported carcinoma, but only atypical ductal hyperplasia. However, at operation a clear skin dimple was noted in the left upper quadrant, strongly suggesting cancer (this clinical sign was perhaps not noted by the clinician). The mammography report was BIRADS IV/V category (highly suspicious).
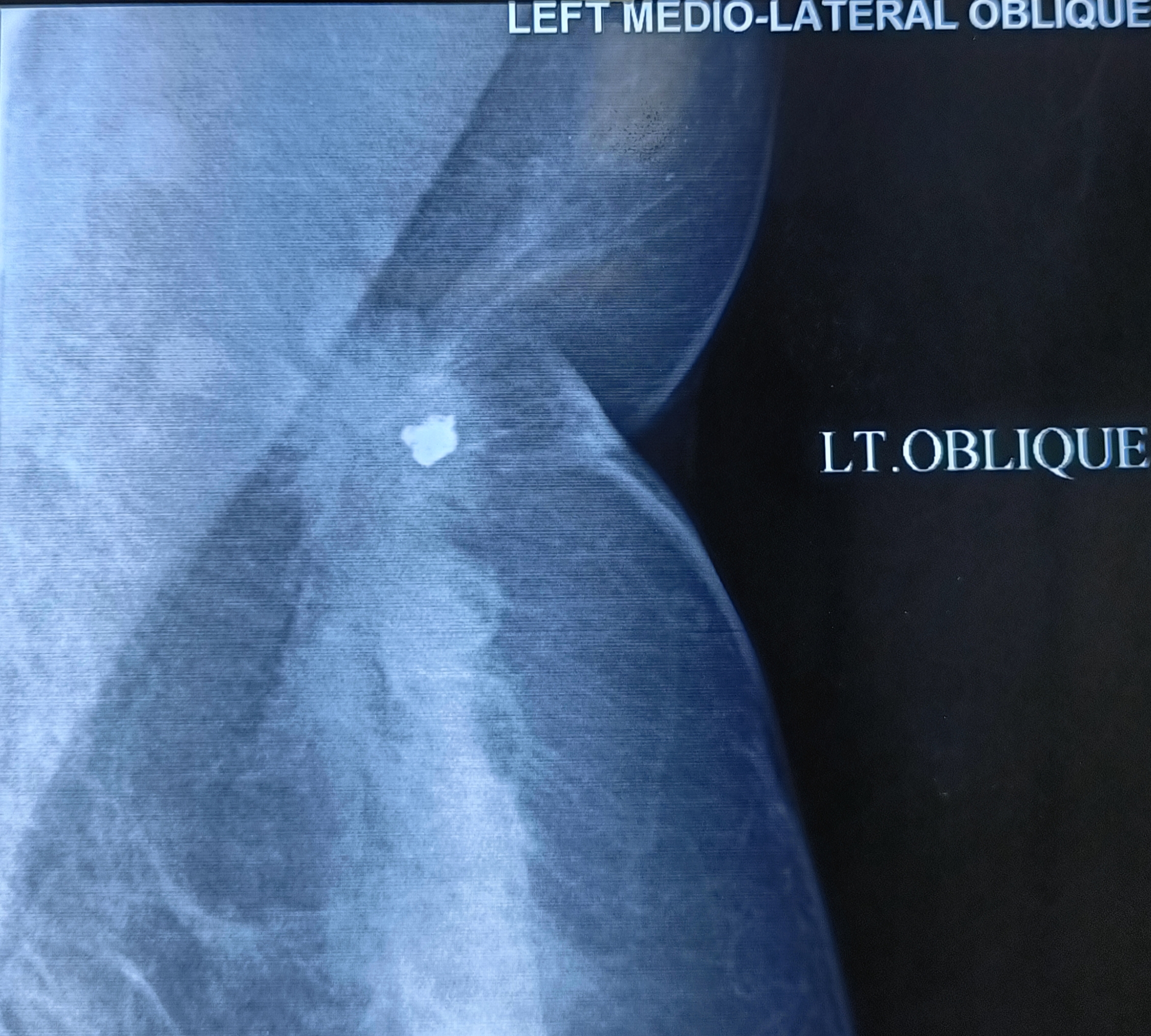


The biopsy report, as expected, was IDC. An MRM was done on 25.5.23.
2.5.23
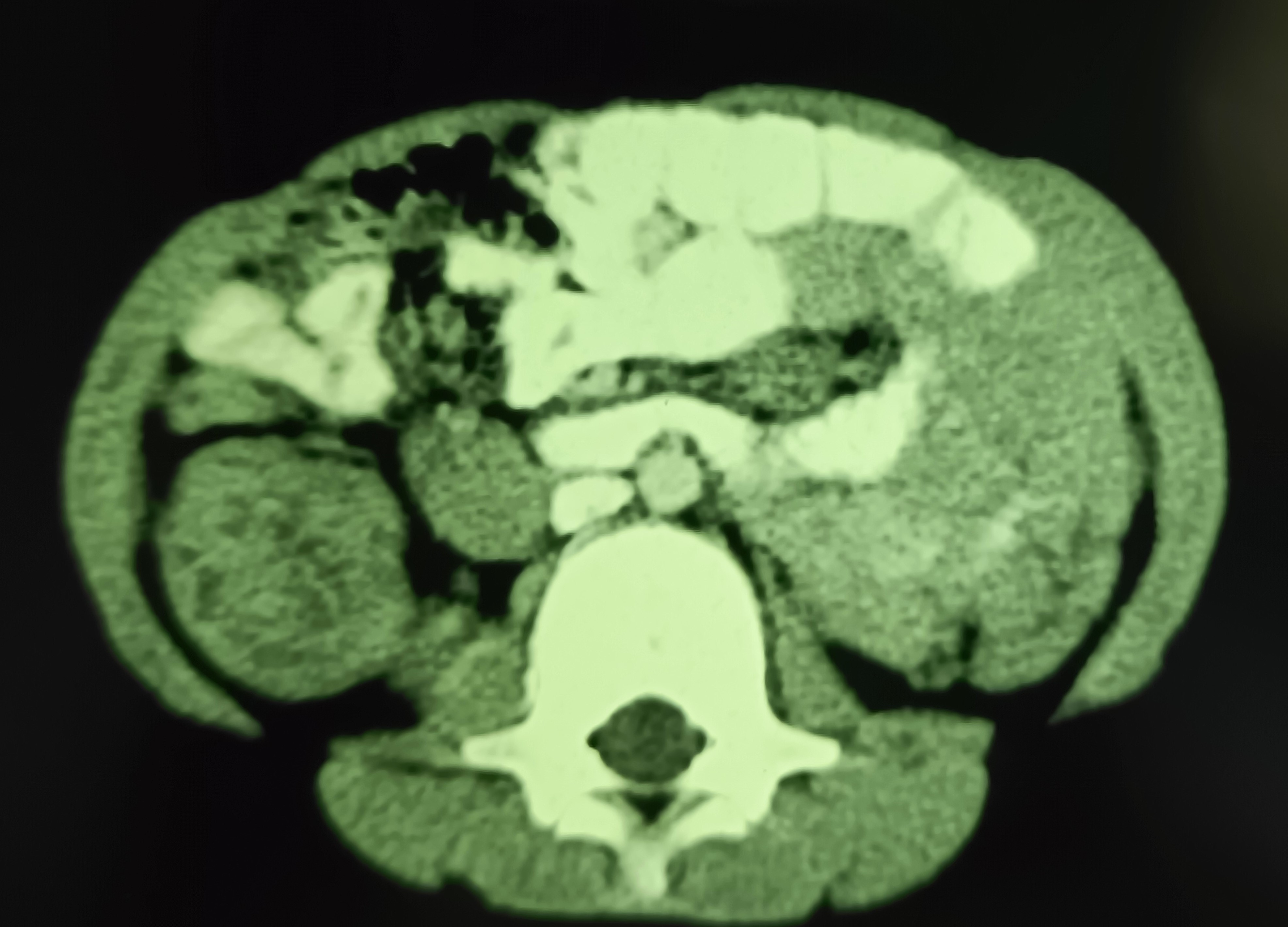
A 7 years old male child admitted with acute abdominal pain showed classic signs of target sign/doughnut sign/pseudo-kidney signs on ultrasound and a mass effect in right iliac fossa on CT. However, the child’s condition improved rapidly and in a few hours he became clinically better and pain free, suggesting spontaneous reduction of the intussusception. Recovered completely on conservative treatment and was not operated.



3.5.23
An elderly man (70 years old), a Nihang, had been having an inguinal hernia for nearly 20 years. This had now grown hugely, extending down into the scrotum, with abdominal X-ray showing signs of intestinal obstruction. However, he was adamant at not having surgery.

12.2.23
A 35 years old female (from Sunam) presented with a chronic left parotid swelling. An ultrasound scan reported a heterogenous mass in the left parotid gland, and a CT scan showed a 22×42 mm sized mass in the superficial lobe; the FNAC suggested chronic reactive lymphoid hyperplasia. At superficial parotidectomy, the superficial lobe was found to be diffusely enlarged (no discrete mass with discrete margins), and was removed. Biopsy reported reactive lymphoid hyperplasia.


